转载:自身免疫性肝炎该如何治疗?
看到一篇文章,分享给大家
1
药物治疗
国际上各大肝病学会均发表了AIH诊疗指南[1,2],指出AIH治疗的目标是同时达到生化学应答(血清氨基转移酶和IgG水平复常)和组织学缓解。表1总结了治疗方案。鉴于有关AIH的随机对照研究相对较少,多数推荐意见来源于专家意见和病例报道。
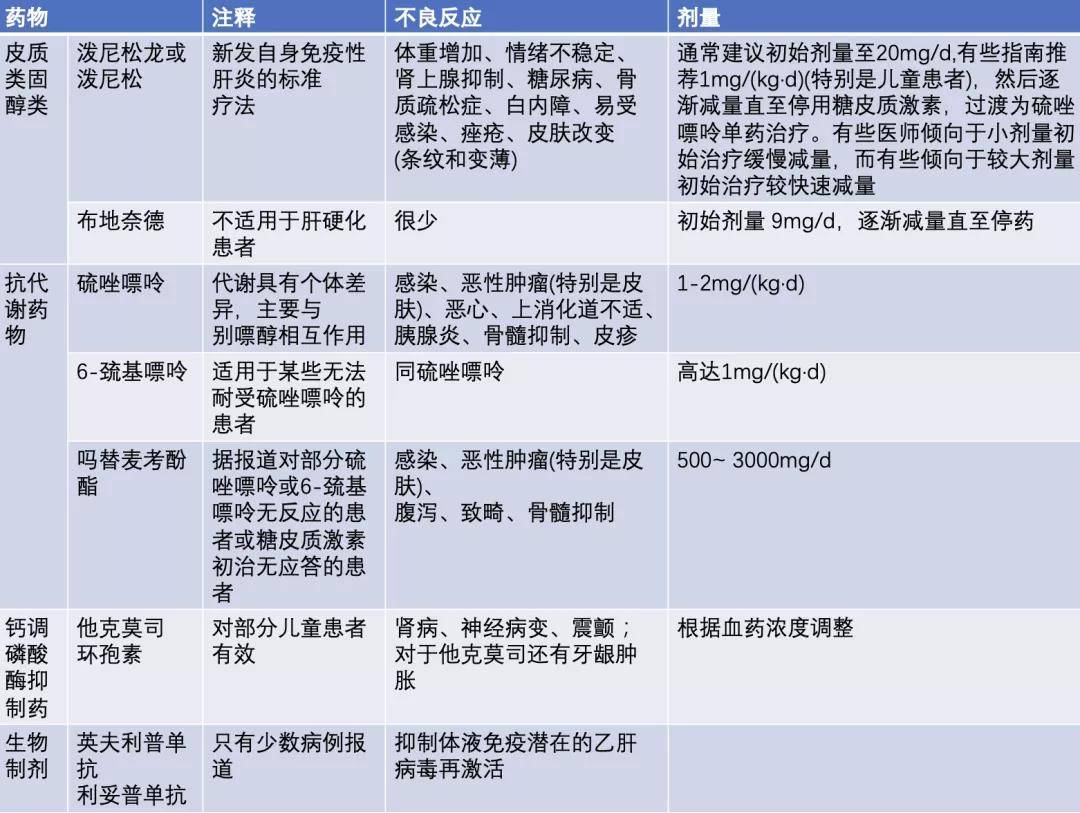
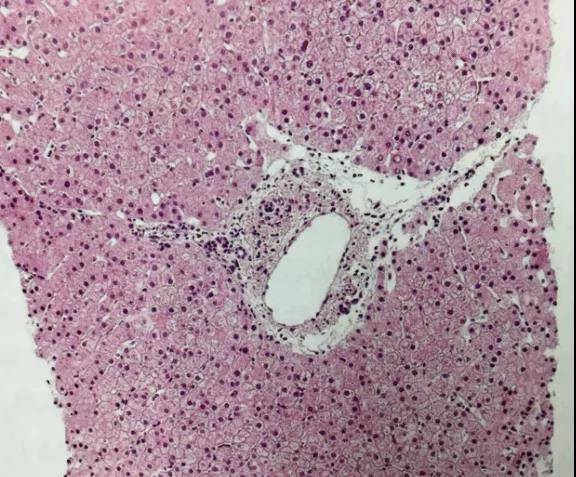
图1. 免疫性肝炎患者经过3年免疫抑制治疗后获得了临床缓解,肝穿刺提示肝组织活检未见异常。
2
肝脏移植
失代偿规肝病或暴发性肝衰竭患者需考虑肝脏移植。术前需要与肝移植团队进行讨论,对免疫抑制治疗与移植的风险-效益比进行个体化评估。一项来自英国的大型系列研究数据显示,约2%的AIH患者需要肝移植[8]。
3
一般注意事项
AIH患者的长期管理包括维持最小有效剂量免疫抑制治疗、对可能出现的不良反应的治疗及对慢性肝病的治疗。
4
预后
AIH通常预后良好,几项队列研究结果显示,包括代偿期肝硬化在内的AIH患者,其生存率与普通人群相似[16]。然而,一项英国队列研究显示,AIH患者的生存率略低于普通人群[8]。尽管具有肝硬化的临床表现并不影响对糖皮质激素治疗的应答,但会影响预后。据报道,2型AIH和SLA/LP阳性者预后较差。
▼参考文献
[1] European Association for the Study of the Liver. EASL clinical practice guidelines: autoimmune hepatitis. J Hepatol 63:971-1004.
[2]Manns MP, Czaja AJ, Gorham JD, et al. Diagnosis and management of autoimmune hepatitis. Hepatology 51:2193- -213.
[3] Cook GC,Mulligan R, Sherlock S. Controlled prospective trial of corticosteroid therapy in active chronic hepatitis. Q J Med 40:159- - 85.
[4] Czaja AJ, Wolf AM, Baggenstoss AH. Laboratory assessment of severe chronic active liver disease during and after corticosteroid therapy: correlation of serum transaminase and gamma globulin levels with histologic features.Gastroenterology 80:687- -92.
[5]Manns MP, Woynarowski M, Kreisel W, et al. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis.Gastroenterology 139:1198- 206.
[6] Murray- -Lyon IM, SternRB,Williams R. Controlled trial of prednisone and azathioprine in active chronic hepatitis. Lancet 1:735- -7.
[7] Heneghan MA, Allan ML, Bornstein JD, Muir AJ, Tendler DA. Utility of thiopurine methyltransferase genotyping and phenotyping, and measurement of azathioprine metabolites in the management of patients with autoimmune hepatitis. J Hepatol 45:584- -91.
[8] Hoeroldt B, McFarlane E, Dube A, et al. Long-term outcomes of patients with autoimmune hepatitis managed at a nontransplant center. Gastroenterology 140:1980- -9.
[9] Zachou K, Gatselis NK, Arvaniti P, et al. Areal. -world study focused on the long- -term efficacy of mycophenolate mofetil as first-line treatment of autoimmune hepatitis. Aliment Pharmacol Ther 43:1035- - 47.
[10] Trivedi PJ, Hirschfield GM. Review article: overlap syndromes and autoimmune liver disease. Aliment Pharmacol Ther 36:517- -33.
[11]Czaja AJ, Carpenter HA. Decreased fibrosis during corticosteroid therapy of autoimmune hepatitis. J Hepatol 40:646- -52.
[12]Schramm C, Bubenheim M, Adam R. Primary liver transplantation for autoimmune hepatitis: a comparative analysis of the European Liver Transplant Registry. Liver Transpl 2010;16(4):461-9.
[13] Montano- -Loza AJ,Mason AL,MaM, Bastiampillai RJ, Bain VG, Tandon P. Risk factors for recurrence of autoimmune hepatitis after liver transplantation. Liver Transpl 15:1254- -61.
[14] Yeoman AD, Al Chalabi T, Karani JB, Quaglia A. Evaluation of risk factors in the development of hepatocellular carcinoma in autoimmune hepatitis: Implications for follow-up and screening. Hepatology 48(3):863- -70.
[15] HeneghanMA, Norris SM, O'Grady JG, Harrison PM,McFarlane IG. Management and outcome of pregnancy in autoimmune hepatitis. Gut 48:97-102.
[16] Roberts SK, Therneau TM, Czaja AJ. Prognosis of histological cirrhosis in type 1 autoimmune hepatitis. Gastroenterology 110:848- 57.
[17] MontanoLoza AJ, Carpenter HA, Czaja AJ. Consequences of treatment withdrawal in type 1 autoimmune hepatitis. Liver Int 27:507-15.
收藏
回复(0)参与评论
评论列表